
Dry Mouth
The medical term for dry mouth is xerostomia. With a dry mouth, you should know it can signal medication side effects, dehydration, diabetes, Sjögren’s syndrome, or oral infections, so you should assess medications and fluid intake and seek medical testing for underlying causes.
Key Takeaways:
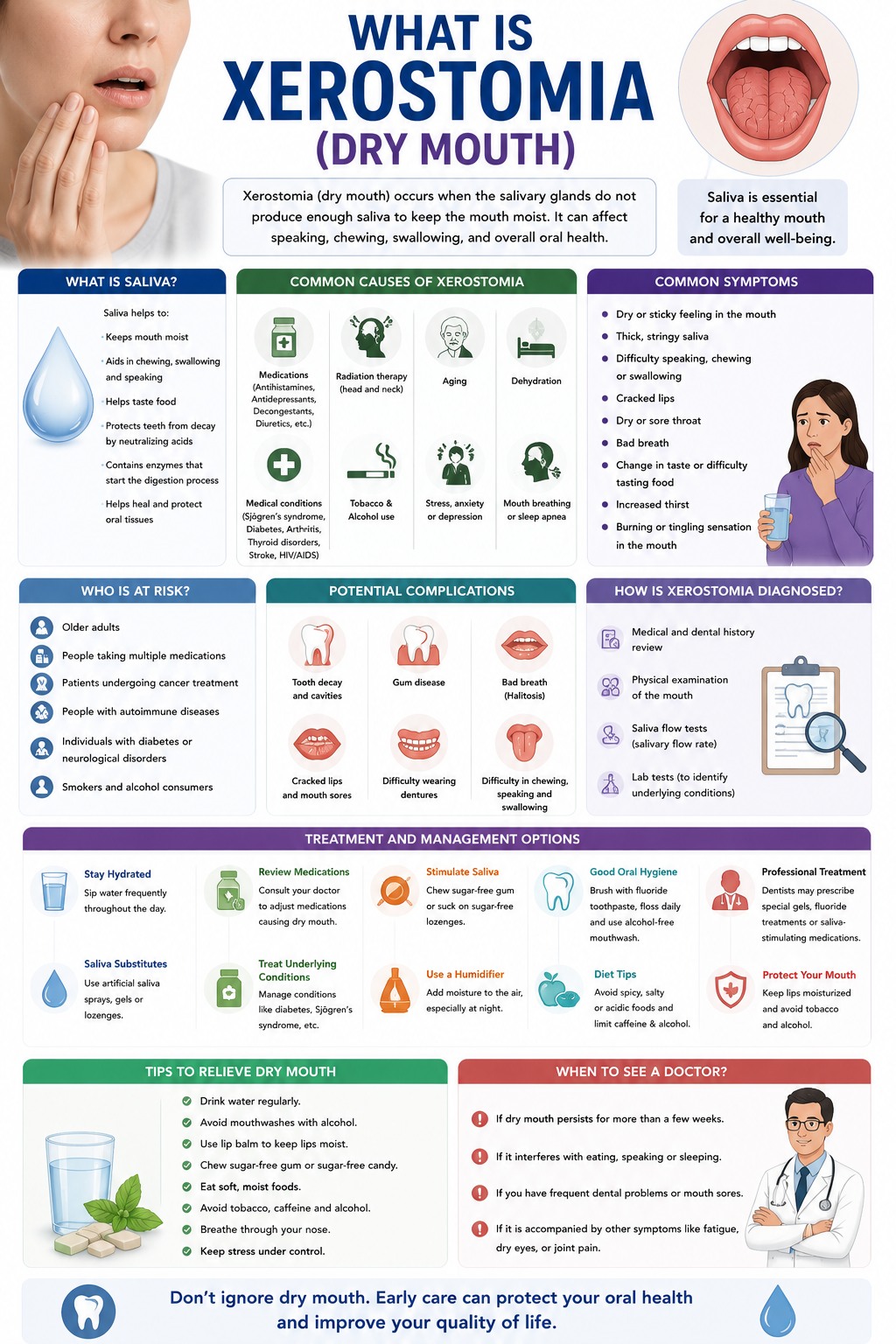
- Common causes of xerostomia include medications, radiation or chemotherapy to the head and neck, dehydration, mouth breathing, diabetes, smoking, and autoimmune diseases.
- Surgery and anesthesia can cause temporary dry mouth via intubation, opioid painkillers, anticholinergic drugs, or nerve injury that reduces salivary gland function.
- Anxiety and acute stress activate the sympathetic nervous system, reducing saliva production and causing transient or persistent dry mouth.
- Concurrent dry mouth and dry eyes suggest Sjögren’s syndrome or other systemic autoimmune conditions and warrant rheumatology evaluation and antibody testing.
- Symptoms include a sticky or cottony feeling, sore throat, bad breath, difficulty chewing or swallowing, altered taste, increased dental decay, oral infections, and cracked lips.
- Conservative treatments include increased water intake, sugar-free gum or xylitol lozenges, saliva substitutes or oral moisturizers, humidifiers, strict oral hygiene, and avoiding alcohol, caffeine, and tobacco; review medications with a clinician for alternatives.
- Complementary options such as acupuncture may relieve radiation-induced xerostomia for some patients; homeopathy and most natural remedies show reliable evidence for burning-mouth or chronic xerostomia and can replace medical evaluation.
Clinical Presentation of Xerostomia and Associated Symptoms
Clinical signs include the classic symptoms of xerostomia, such as sticky oral mucosa, tongue fissuring, and a sensation of cottonmouth that you will notice during speech and swallowing.
You may also experience increased dental caries, halitosis, altered taste perception, and frequent throat clearing that reflect reduced salivary protection and ongoing mucosal irritation.
Saliva quantity and quality decline can coincide with systemic complaints; when you report dry mouth and eyes together, document medication changes, autoimmune history, and timing to guide evaluation.
Identifying common symptoms of dry mouth
Dry lips, persistent thirst, and a need to sip liquids when eating are among the most reported symptoms of xerostomia that you should track daily for patterns and triggers.
Common functional effects include difficulty speaking for long periods, trouble wearing dentures, and nocturnal mouth breathing that disrupts sleep and worsens oral discomfort for you.
Frequent oral infections like candidiasis, increased tooth sensitivity, and a burning tongue often accompany the symptoms of dry mouth and warrant prompt dental and medical review by you.
The physiological correlation between dry mouth and eyes
Correlating salivary gland hypofunction with lacrimal gland involvement explains why xerostomia and eyes appear together in disorders such as Sjögren’s syndrome, which you should consider when both sites are affected.
Eye dryness produces a gritty sensation, photosensitivity, and blurred vision that mirror oral mucosal fragility; when you experience both, inflammatory processes or medication effects may be driving the symptoms.
When evaluating overlap, measure tear breakup time and unstimulated salivary flow so you can quantify severity and discuss targeted treatments addressing dry mouth and eyes with your clinician.
Further testing like anti-Ro/SSA and anti-La/SSB antibodies, along with Schirmer’s test and salivary gland imaging, can help you distinguish primary autoimmune causes from drug-induced or age-related declines in gland function.
Etiology and Underlying Causes of Xerostomia
You should review. What causes xerostomia? Dry mouth causes and reasons for dry mouth are the primary checklist items when evaluating xerostomia, as medication effects, systemic diseases, and behavioral factors often explain the decline in salivary flow.
Medication side effects commonly explain persistent dryness; antihistamines, anticholinergics, certain antidepressants and some antihypertensives reduce salivary flow, so you will need to audit prescriptions and over-the-counter agents for contributors.
Autoimmune conditions such as Sjögren’s syndrome, head and neck radiation, uncontrolled diabetes and chronic dehydration are frequent underlying causes, and you should correlate symptoms with clinical history, oral exam and basic labs.
Analyzing primary dry mouth causes and triggers
Analyzing your daily medications and supplements reveals common culprits, with antimuscarinics and tricyclic antidepressants among the most often implicated, so you should flag any drugs known to cause xerostomia.
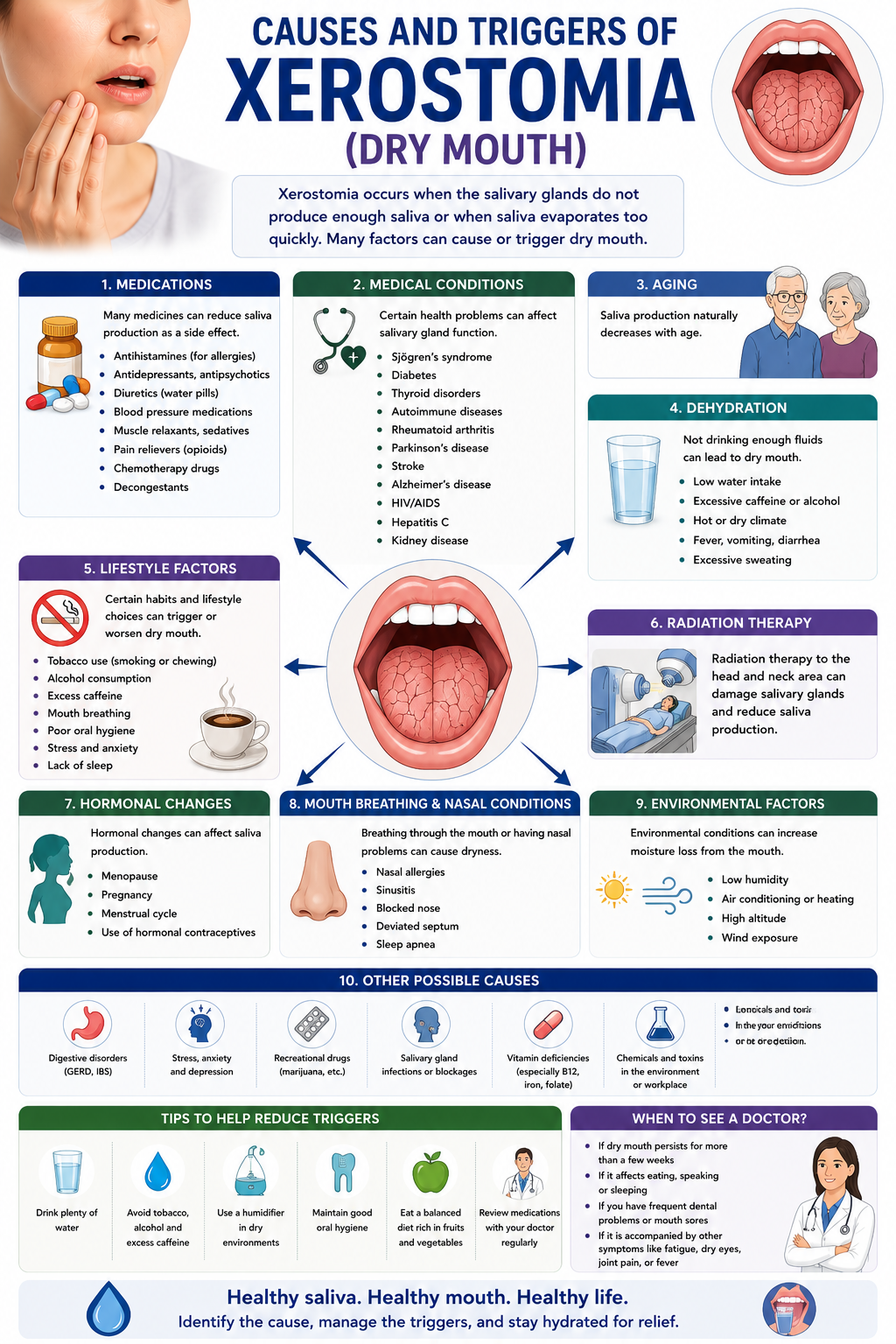
Drugs and lifestyle choices also act as triggers: tobacco, alcohol, high caffeine intake and recreational cannabis can exacerbate dryness, and you should assess consumption patterns and breathing habits that increase mouth drying.
Age and polypharmacy frequently combine to produce symptoms; therefore, you should review comorbidities, recent medication changes and signs of systemic disease when pinpointing primary causes.
Investigating various physiological reasons for dry mouth
Investigating salivary gland hypofunction involves considering acinar cell loss, ductal obstruction, and autonomic neuropathy, and you should request sialometry or imaging when a physical exam suggests gland impairment.
Radiation-induced gland damage after head and neck cancer treatment often produces prolonged xerostomia, so you should document any history of radiotherapy and correlate timing and dose with symptom onset.
Hormonal shifts, especially during menopause, and metabolic disorders such as diabetes with autonomic neuropathy can reduce salivary output, and you should include endocrine evaluation where clinical context indicates.
Salivary testing, targeted imaging and trials of sialogogues or saliva substitutes help confirm physiological causes, so you should pursue objective measures and specialist referral when conservative measures fail.
Impact of Medical Procedures and Mental Health for Xerostomia Development
Surgery often leaves you with dry mouth after surgery because general anesthesia, opioid pain medications, and intubation reduce saliva production and alter oral flora; you may notice thick saliva, cracked lips, or a coated tongue within the first 24-72 hours.
After dental extractions or major operations you should watch for medication-related xerostomia, since anticholinergics and sedatives commonly intensify dryness and raise the risk of oral infections and tooth decay if hydration and hygiene lapse.
You will also encounter anxiety and dry mouth when stress spikes sympathetic tone, which lowers salivary flow and can compound postoperative discomfort unless both physical and mental health factors are addressed.
Managing oral complications and dry mouth after surgery
Managing xerostomia after surgery requires frequent sips of water, saliva substitutes, and sugar-free lozenges and avoiding alcohol or tobacco; your surgical team can modify offending medications and recommend topical fluoride to prevent decay.
Follow postoperative instructions for oral suctioning, wound hygiene, and pain control, and report any ongoing dryness so providers can check for fungal overgrowth or change anticholinergic therapies.
Ensure you attend scheduled follow-ups and discuss saliva-stimulating options like pilocarpine only under medical supervision, since dosing must align with your overall recovery and comorbidities.
The systemic link between anxiety and dry mouth
Anxiety causes sympathetic activation, so you feel anxiety and xerostomia because of reduced salivary flow, increased oral discomfort, and xerostomia that can disrupt sleep and nutrition during recovery.
When you live with chronic anxiety, repeated episodes of dry mouth increase the chance of dental erosion and gingival problems because saliva’s buffering and antimicrobial actions are diminished.
Stress reduction techniques like progressive breathing, CBT, and biofeedback, along with short-term targeted pharmacotherapy when needed, can reduce dry mouth by calming the fight-or-flight response that lowers saliva.
Research indicates that coordinating mental health care with dental and surgical follow-up helps you address both psychological triggers and oral consequences of anxiety and dry mouth, so arrange collaborative care among your dentist, surgeon, and therapist.
Holistic and Integrative Treatment Modalities for Dry Mouth
Holistic approaches combine dietary adjustments, hydration strategies, and targeted over-the-counter options, and you should consider natural remedies for dry mouth such as xylitol lozenges, aloe vera rinses, or sugar-free gum while confirming safety with your clinician.
Integrative care often pairs lifestyle changes with acupuncture for xerostomia, using acupuncture to modulate autonomic tone and salivary function while continuing oral moisturizing agents under the guidance of a practitioner.
Coordination between your dentist, primary care provider, and licensed acupuncturist helps you sequence treatments, monitor side effects from any natural remedy for dry mouth, and evaluate objective measures like unstimulated salivary flow rates.
Selecting an effective natural remedy for dry mouth
Choosing a natural remedy for xerostomia starts with a symptom diary and a review of medical history so you can safely try options such as xylitol lozenges, aloe vera rinses, or herbal glycerin sprays under clinical supervision.
Assess product quality by checking ingredient lists, avoiding added sugars, verifying third-party testing when possible, and tracking changes in dry mouth severity over two to four weeks to determine whether the remedy is working for you.
Monitor for side effects like gastrointestinal upset from sugar alcohols or allergic reactions to botanicals and discontinue the natural remedy for dry mouth if symptoms worsen, reporting outcomes to your clinician for next-step planning.
Clinical applications of acupuncture for dry mouth
Acupuncture for dry mouth commonly targets points such as LI4 (Hegu), ST6 (Jiache), ST7 (Xiaguan), and SJ17 (Yifeng), and you may see improved salivary flow after a course of 6-10 sessions delivered twice weekly.
Evidence for acupuncture for dry mouth includes clinical reports and smaller trials indicating symptomatic relief and measurable increases in unstimulated salivary flow, so you should seek licensed practitioners who document objective outcomes.
Protocol customization matters because needle placement, choice of manual versus electroacupuncture, and session frequency affect the results; therefore, you should expect individualized plans and informed consent before starting treatment.
Follow-up assessments should measure unstimulated and stimulated salivary rates, patient-reported dryness scales, and any interactions with concurrent natural remedy for dry mouth therapies to guide ongoing care and treatment adjustments.
Homeopathic Protocols for Chronic Oral Dryness
In practice, you can add individualized remedies to homeopathy for xerostomia after detailed case-taking that looks at medication history, autoimmune markers, and symptom timing; common constitutional choices reported by practitioners include Bryonia alba, Natrum muriaticum, and Arsenicum album, often trialed in 6C or 30C under supervision.
Clinical guidance suggests combining saliva-stimulating measures and topical care with homeopathy for dry mouth, using repertorization to match modalities such as worse on swallowing or at night and assessing response across a 4-8 week window before adjusting prescriptions.
Patients who report burning sensations need separate tracking because homeopathy for burning dry mouth may require remedies focused on neuropathic descriptors or coexisting oral candidiasis, and you should coordinate with conventional testing when indicated.
Targeted applications of homeopathy for dry mouth
Targeted interventions in homeopathy for xerostomia include lozenge-based delivery, low-dose oral tinctures, and constitutional prescriptions tailored to causes like Sjögren’s or post-radiation xerostomia, with specificity driven by symptom onset and pattern.

You should collaborate with a trained homeopath to select remedies; practitioners commonly consider Bryonia, Pulsatilla, Lachesis and Calcarea carbonica for distinct dry-mouth presentations rather than applying a single standard formula.
Individual monitoring through symptom diaries and objective measures helps you and your practitioner decide whether homeopathy for dry mouth is reducing dryness, improving taste, or altering burning sensations and when adjunctive therapies are needed.
Specialized homeopathy for burning dry mouth sensations
Specialized remedy choices for homeopathy for burning dry mouth emphasize agents known for addressing burning quality: Arsenicum album for intense burning, Phosphorus for raw heat, and low-potency Capsicum for localized burning sensations, selected via detailed symptom description.
Many clinicians vary potencies from 6C to 200C depending on chronicity and sensitivity; you may receive a single-dose constitutional prescription with follow-up observation for 1-4 weeks before repeating or altering the remedy.
When burning dry mouth coexists with metallic taste, oral soreness or neuropathic features, a focused homeopathic strategy can be combined with saliva substitutes and antifungal assessment to create a comprehensive plan you can follow.
Lastly, you should document triggers such as spicy foods, mouth breathing or medication changes and report objective data like unstimulated salivary flow or Sjögren’s serology so that homeopathy for burning dry mouth is integrated safely with conventional diagnostics.
Conclusion
As a reminder, you should evaluate the cause of xerostomia and select evidence-based dry mouth treatment and dry mouth remedies such as saliva substitutes, sugar-free lozenges, prescription sialogogues, and topical gels to restore oral comfort and protect enamel.
You should address medication side effects, increase plain water intake, limit caffeinated and alcoholic beverages, and maintain meticulous oral hygiene with fluoride toothpaste and alcohol-free mouthwash to reduce caries risk and mucosal cracking.
Follow-up with your dentist or physician for objective testing, implement holistic treatments where appropriate (hydration protocols, saliva-stimulating gum, or behavioral breathing techniques), and adjust care until symptoms improve.

FAQ

Q: What is dry mouth (xerostomia) and how does it affect oral health?
A: Dry mouth, medically called xerostomia, is a subjective feeling of reduced saliva. Saliva protects teeth, helps digestion, controls bacteria, and keeps oral tissues moist; persistent reduction raises risks of cavities, oral infections, difficulty swallowing, altered taste, and cracked lips.
Q: What are the most common causes of dry mouth?
A: Anticholinergic or sympathomimetic drugs are the most common cause. These include antihistamines, decongestants, antidepressants, antipsychotics, and some blood pressure drugs. Radiation to the head and neck, chemotherapy, systemic diseases such as diabetes and Sjögren’s syndrome, dehydration, mouth breathing, smoking, and nerve damage from surgery or trauma also reduce saliva production.
Q: What symptoms suggest my dry mouth needs medical evaluation?
A: Symptoms include persistent oral dryness, difficulty speaking or swallowing, frequent thirst, sticky or stringy saliva, burning sensations, altered taste, and increased cavities or oral infections. Concurrent signs such as dry eyes, joint pain, unexplained fatigue, high blood sugar, or rapid weight loss suggest an underlying systemic condition that warrants prompt medical assessment.
Q: Why do people experience dry mouth after surgery and how can it be managed?
A: General anesthesia, endotracheal intubation, perioperative anticholinergic drugs, opioids, and post-op mouth breathing commonly cause temporary dry mouth. Management includes sipping water, using saliva substitutes or oral moisturizers, chewing sugar-free gum when safe, humidifying the environment, and reviewing medications with the care team if symptoms persist beyond the expected recovery period.
A: Anxiety triggers sympathetic nervous system activation that suppresses salivary flow, producing a dry-mouth sensation. Holistic measures include slow diaphragmatic breathing, progressive muscle relaxation, cognitive-behavioral techniques or therapy, regular hydration, chewing sugar-free gum or xylitol lozenges to stimulate saliva, avoiding excessive caffeine and alcohol, and maintaining optimal sleep and exercise habits.
Q: Is dry mouth combined with dry eyes a sign of Sjögren’s syndrome and how is it evaluated?
A: Concurrent dry mouth and dry eyes raise suspicion for Sjögren’s syndrome, an autoimmune disorder targeting moisture-producing glands. Evaluation usually includes blood tests for antibodies (anti-Ro/SSA, anti-La/SSB), objective tear tests (Schirmer), salivary flow measurement or imaging, and sometimes a minor salivary gland biopsy; management may include saliva stimulants, topical therapies, immunomodulatory care, and coordinated rheumatology and dental follow-up.
Q: What holistic, natural, and alternative treatments help dry mouth, and do acupuncture or homeopathy work for burning, dry mouth?
A: Practical natural remedies with supportive evidence include frequent sipping of water, sugar-free gum or xylitol lozenges to stimulate saliva, alcohol-free mouthwashes, saliva substitutes and oral moisturizers, humidifiers at night, strict oral hygiene, and avoiding tobacco, alcohol, and high-caffeine drinks. Acupuncture has shown modest benefits in some trials for radiation-induced xerostomia, but results are mixed and technique-specific. High-quality evidence does not support homeopathy as an effective treatment for xerostomia or burning-mouth symptoms; homeopathic remedies should not replace medical evaluation. For persistent burning sensations or severe xerostomia, consult a clinician for diagnostic testing and treatments such as prescription saliva stimulants (pilocarpine or cevimeline) or targeted neuropathic therapies when appropriate.
Holistic Treatment for Xerotomia in Philadelphia
If you choose natural xerotomia treatment, ensure you follow the recommendations of a good and well-trained medical professional.
At the Philadelphia Homeopathic Treatment Center, Dr. Tsan and associates use the most effective approaches to natural treatment for dry mouth. Thus, the effectiveness of xerotomia treatment here is approximately 10% higher than the nationwide average.
Contact the clinic at (267) 403-3085 or use our online application to make your appointment with Doctor Tsan and start your treatment.