Hypogonadism
Just because your body isn’t producing enough testosterone or estrogen doesn’t mean you’re alone—hypogonadism affects men and women when the sex glands generate few or no hormones. This condition can stem from issues in the testes, ovaries, pituitary gland, or hypothalamus, leading to symptoms like fatigue, low libido, infertility, and mood changes. You can explore natural approaches alongside medical guidance to support hormonal balance.
Key Takeaways:
- Hypogonadism occurs when the body doesn’t produce enough sex hormones due to problems in the testes or ovaries, or in the brain regions that regulate them—mainly the hypothalamus and pituitary gland.
- There are two main types: primary hypogonadism, where the issue lies in the gonads themselves, and secondary (or hypogonadotropic) hypogonadism, which stems from dysfunction in the hypothalamus or pituitary.
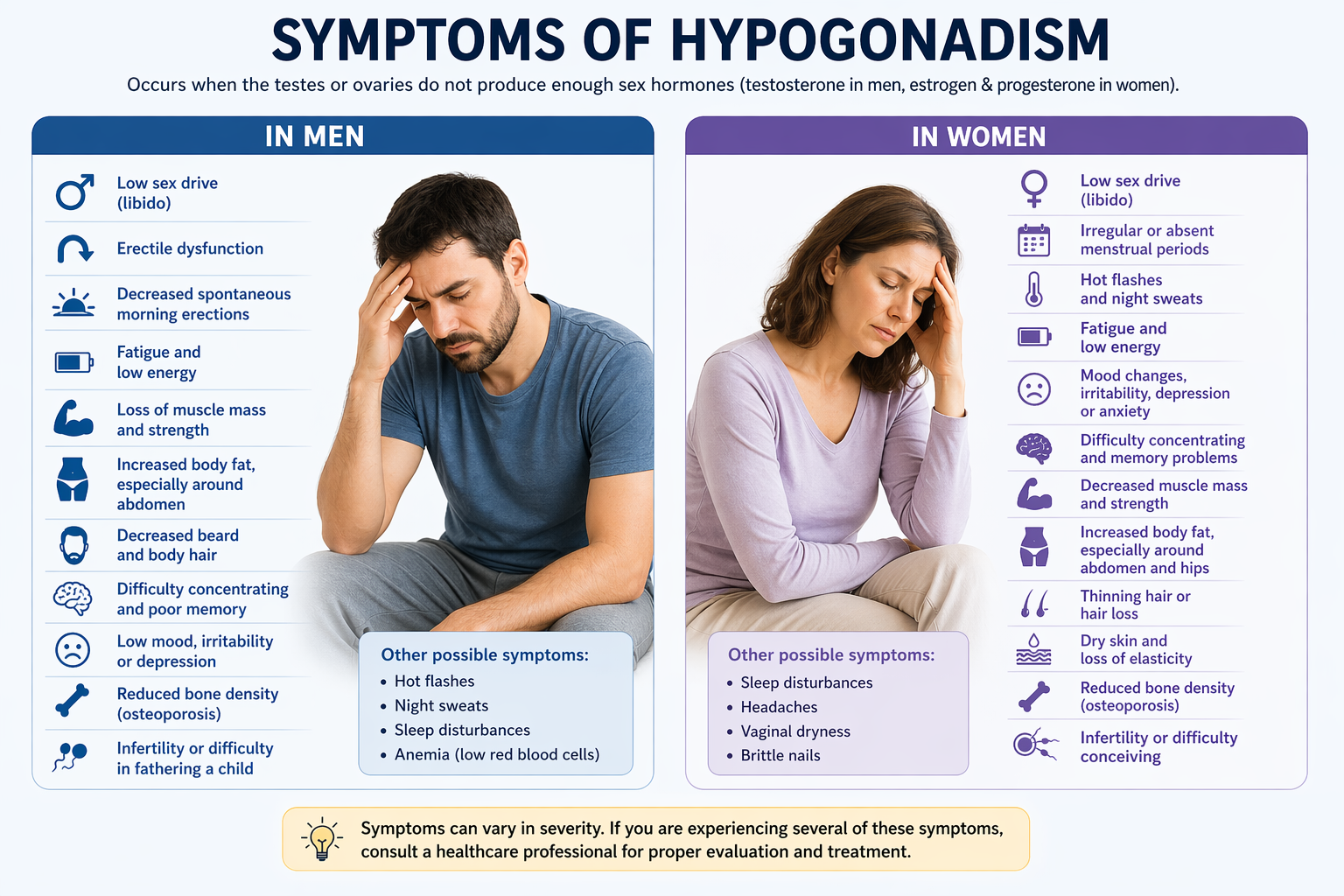
- Men with hypogonadism may experience low libido, fatigue, reduced muscle mass, and infertility, while women may face irregular periods, hot flashes, and trouble conceiving.
- Common causes of primary hypogonadism include genetic conditions like Klinefelter syndrome in men or Turner syndrome in women, testicular or ovarian injury, and autoimmune disorders.
- Diagnosis typically involves blood tests to measure hormone levels such as testosterone, estrogen, FSH, and LH, along with imaging or genetic testing when needed.
- Hormone replacement therapy is a common part of treatment, but some people look into natural ways to help balance hormones, such as getting better sleep, managing stress, getting more exercise, and eating better.
- Although scientific evidence is scarce, some individuals claim to experience benefits from complementary therapies such as acupuncture or homeopathy; however, these should not supplant medical assessment or treatment.
Classification and Types of the Hypogonadism
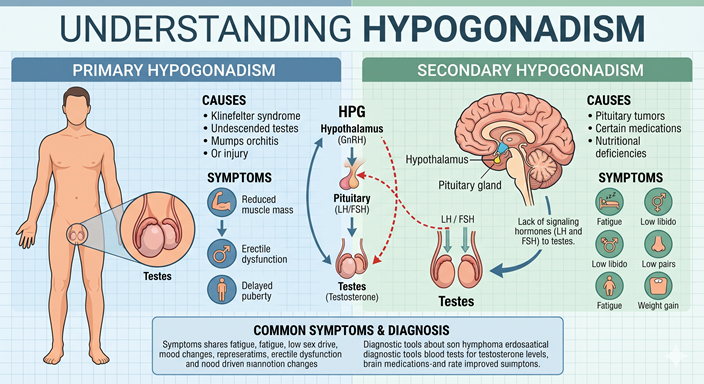
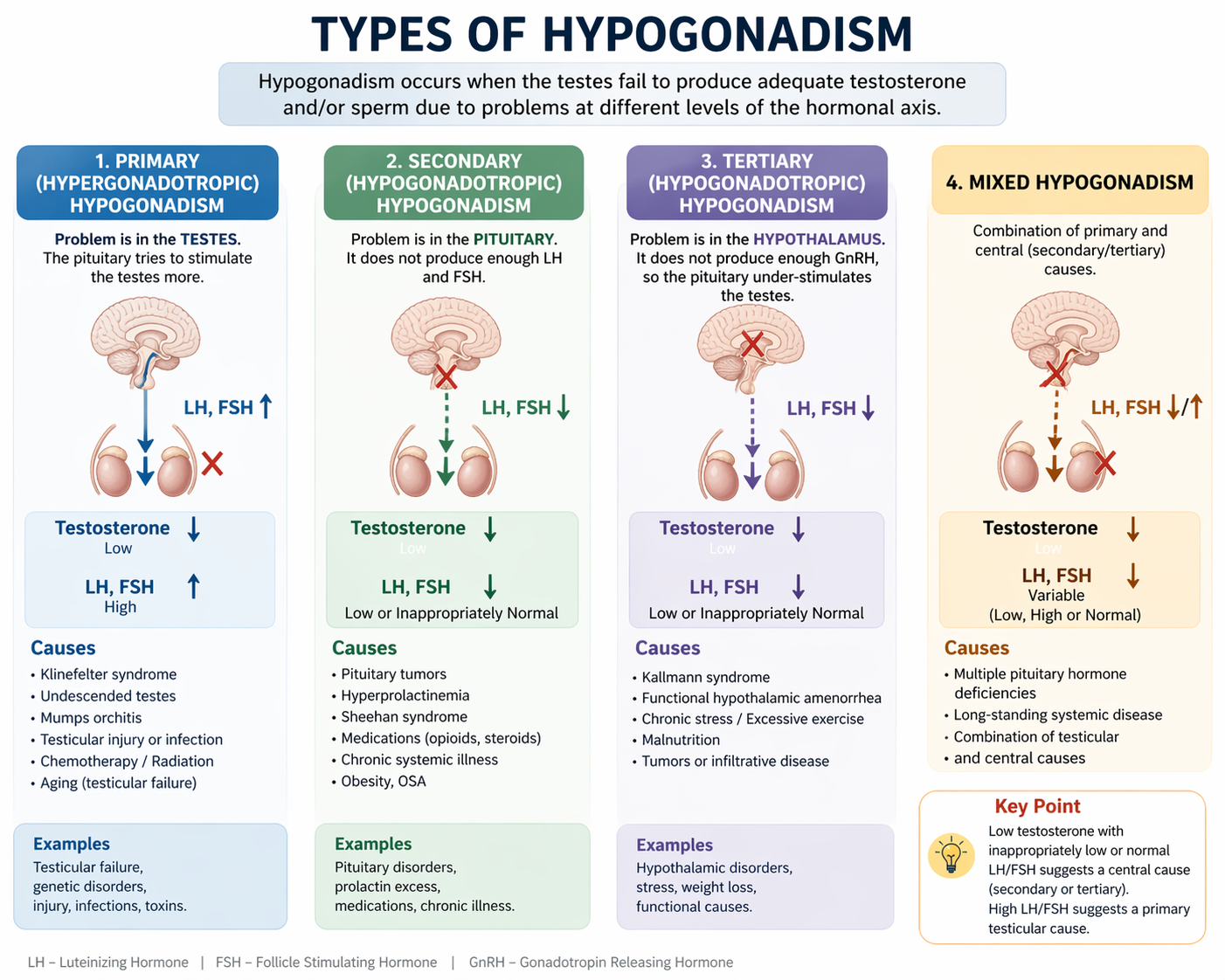
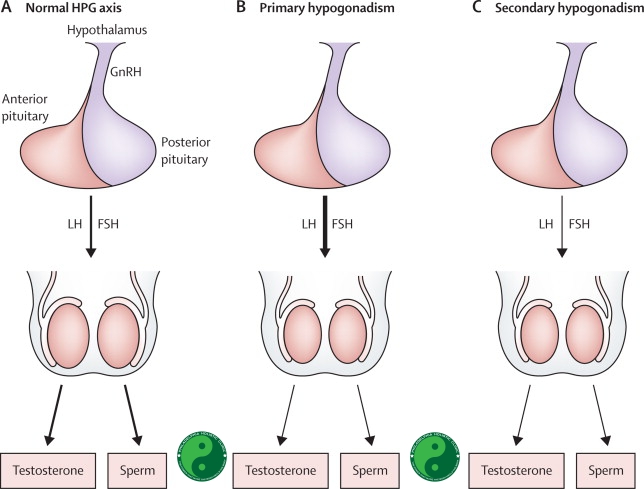
Hypogonadism is broadly categorized into two main types: primary and secondary, each defined by where the dysfunction occurs in the hormonal pathway. Primary hypogonadism arises when the testes or ovaries fail to produce adequate sex hormones despite sufficient stimulation from the pituitary gland. Secondary hypogonadism, in contrast, stems from inadequate signaling from the hypothalamus or pituitary, leading to reduced stimulation of the gonads. These distinctions are further clarified through laboratory markers, particularly levels of luteinizing hormone (LH) and follicle-stimulating hormone (FSH), which help differentiate between hypergonadotropic and hypogonadotropic forms.
Hypergonadotropic hypogonadism is synonymous with primary hypogonadism, marked by elevated LH and FSH due to the gonads’ failure to respond. Causes include genetic conditions like Klinefelter syndrome in males or Turner syndrome in females, as well as testicular injury or chemotherapy. Hypogonadotropic hypogonadism aligns with secondary hypogonadism, showing low or normal gonadotropins alongside low sex hormones. After reviewing your hormone panel, clinicians can pinpoint the origin of dysfunction based on these patterns.
The classification of hypogonadism is best understood through a comparative framework:
| Type | Key Feature |
|---|---|
| Primary Hypogonadism | Hypergonadotropic: high LH/FSH, low sex hormones |
| Secondary Hypogonadism | Hypogonadotropic: low/normal LH/FSH, low sex hormones |
| Hypergonadotropic Hypogonadism | Gonadal failure (e.g., Klinefelter syndrome) |
| Hypogonadotropic Hypogonadism | CNS signaling defect (e.g., Kallmann syndrome) |
| Clinical Diagnosis | Relies on hormone assays and clinical history |
- Primary hypogonadism results in high gonadotropin levels
- Secondary hypogonadism shows low or inappropriately normal LH and FSH
- Hypergonadotropic hypogonadism indicates gonadal failure
- Hypogonadotropic hypogonadism reflects central nervous system dysfunction
After evaluating your hormonal profile and medical history, your provider can determine whether your condition is primary or secondary in origin.
Understanding Primary and Hypergonadotropic Distinctions in Primary Hypogonadism
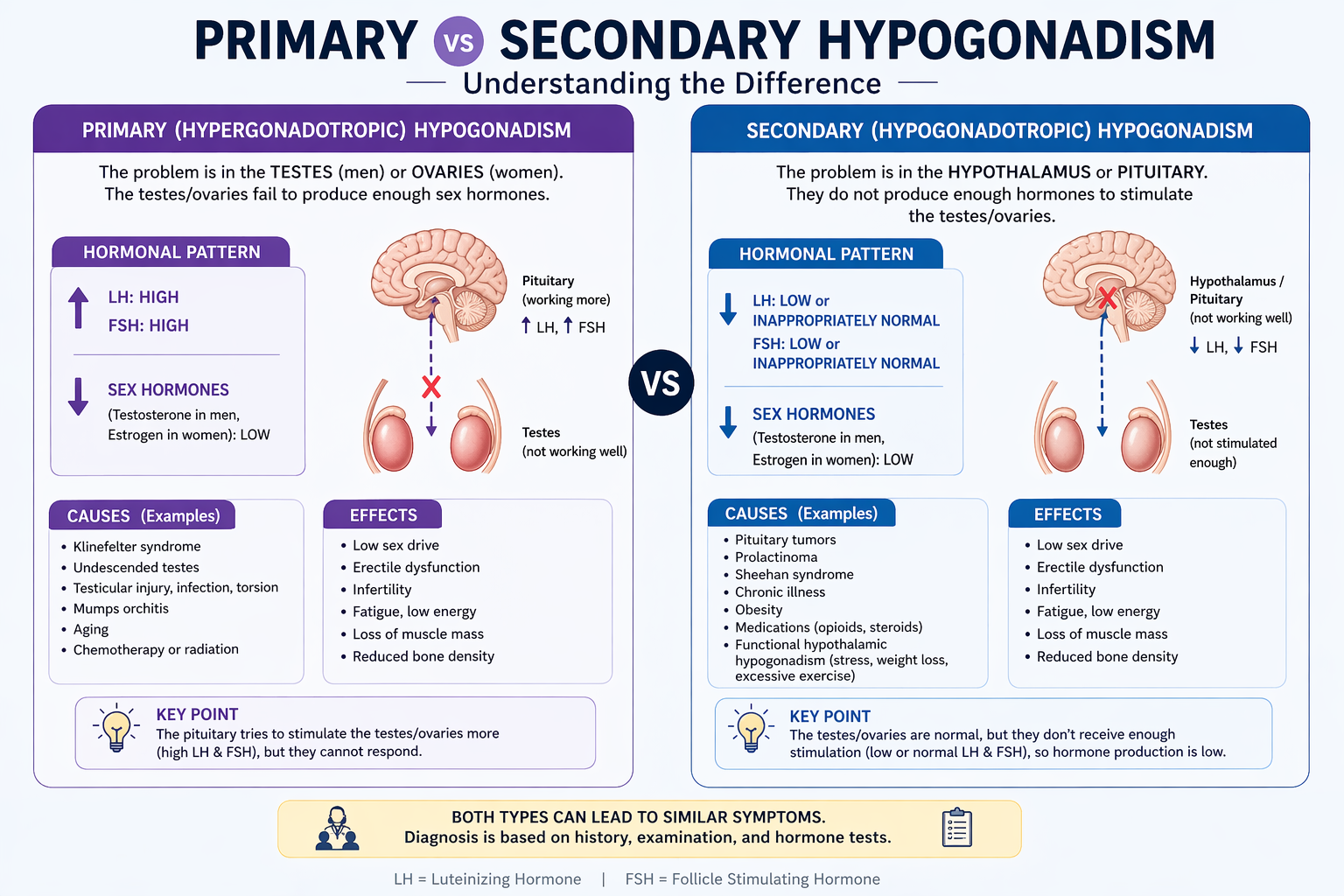
Primary hypogonadism happens when the gonads are not working properly and can’t make testosterone or estrogen, even though they are getting the right signals from the pituitary. This form is labeled hypergonadotropic because the pituitary responds to low sex hormone levels by increasing secretion of LH and FSH, resulting in elevated blood concentrations. Common causes include genetic disorders such as Klinefelter syndrome (47,XXY), which affects approximately 1 in 600 males, or ovarian insufficiency in females linked to Turner syndrome (45,X). Infections like mumps orchitis, radiation, or chemotherapy can also cause permanent gonadal failure.
Your body’s feedback loop is key to understanding this type: when the testes or ovaries underperform, the pituitary attempts to compensate by releasing more stimulating hormones. This results in a clear lab pattern—low sex hormones alongside high LH and FSH—making hypergonadotropic hypogonadism relatively straightforward to diagnose. Unlike reversible forms, primary hypogonadism is often lifelong, requiring ongoing hormone replacement to maintain secondary sexual characteristics, bone health, and fertility support when possible.
Management focuses on restoring hormonal balance through exogenous testosterone or estrogen therapy, tailored to your age, symptoms, and reproductive goals. After diagnosis, regular monitoring ensures optimal dosing and minimizes risks like polycythemia or cardiovascular strain. Assisted reproductive technologies may provide options in select cases, such as sperm retrieval in Klinefelter patients, despite the typical compromise in fertility.
Secondary Gonadal Failure and Hypogonadotropic Mechanisms
Secondary hypogonadism originates not in the gonads but in the brain’s hormonal control centers—the hypothalamus or pituitary.
Gender-Specific Manifestations of Hypogonadism
Physiological Impact on Males
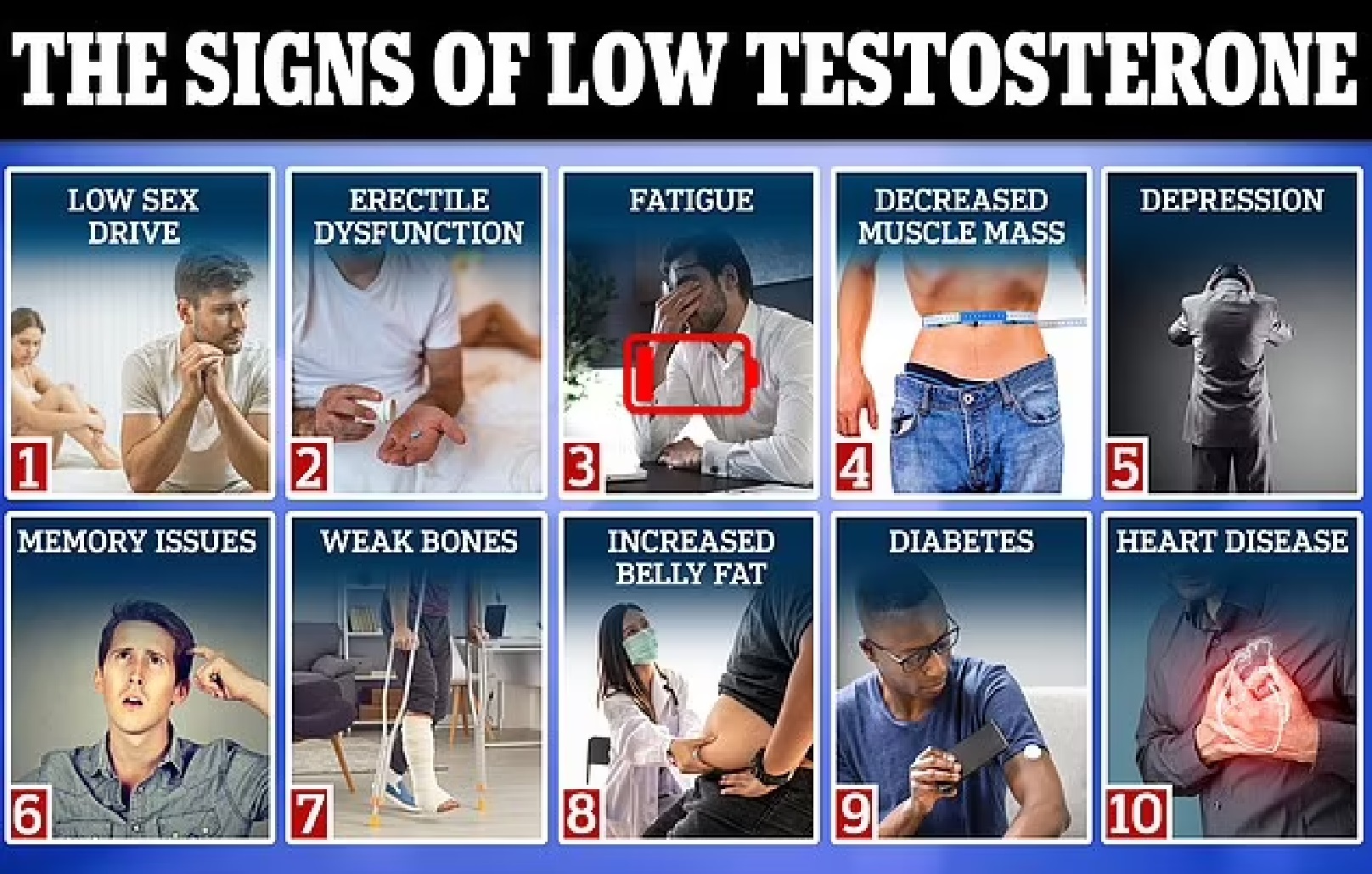
You may notice declining testosterone levels as early as age 30, with hypogonadism in male individuals affecting approximately 2-5% of men overall. This condition disrupts sperm production, often leading to infertility, reduced libido, and erectile dysfunction. Low testosterone also contributes to decreased muscle mass, increased body fat, and fatigue, altering physical performance and daily energy.
Primary or secondary hypogonadism can happen in men when their testicles don’t work right or their pituitary glands don’t. Each type has its own hormonal profile. Symptoms like gynecomastia, reduced facial hair, and testicular atrophy may appear gradually, making early detection difficult without blood testing. Physicians typically measure testosterone levels in the morning, with values below 300 ng/dL indicating potential deficiency.
Chronic conditions such as obesity, type 2 diabetes, and sleep apnea elevate the risk of developing hypogonadism in male adults. Certain medications, including opioids and glucocorticoids, also suppress the hypothalamic-pituitary-gonadal axis. Addressing underlying health issues often improves hormonal balance without the immediate need for exogenous testosterone.
Physiological Impact on Females
Hypogonadism in female individuals results in insufficient estrogen production, disrupting menstrual cycles and often causing amenorrhea. You might experience hot flashes, vaginal dryness, and reduced bone density, increasing long-term risk for osteoporosis. This condition also affects mood and sexual health, contributing to irritability and low arousal.
Primary ovarian insufficiency, affecting 1% of women under 40, is a common cause of hypogonadism in female patients. Autoimmune disorders, genetic conditions like Turner syndrome, or chemotherapy exposure can trigger early ovarian failure. Blood tests revealing elevated FSH levels alongside low estradiol confirm the diagnosis.
Secondary causes stem from hypothalamic or pituitary dysfunction, often linked to excessive exercise, eating disorders, or stress. These factors suppress GnRH release, halting the hormonal cascade needed for ovulation. Restoring energy balance and reducing physical strain may reverse symptoms naturally in some cases.
Women with hypogonadism in female populations often face misdiagnosis due to overlapping symptoms with perimenopause or depression. Early intervention is key to preserving fertility and preventing cardiovascular and skeletal complications. Hormone replacement therapy, when appropriate, can alleviate symptoms while addressing root causes and improve long-term outcomes.
Etiology of Gonadal Failure: Glandular Dysfunction
Primary hypogonadism arises when the testes fail to produce adequate testosterone despite normal stimulation from the hypothalamus and pituitary gland. This disruption originates within the gonads themselves, often due to genetic conditions such as Klinefelter syndrome, where males are born with an extra X chromosome (47,XXY), affecting approximately 1 in 500 to 1,000 male births. Infections like mumps orchitis, particularly when contracted post-puberty, can also inflict direct damage to testicular tissue, impairing hormone production. Autoimmune diseases can attack the testes, causing inflammation and a slow loss of function. Exposure to environmental toxins, including pesticides and industrial chemicals such as phthalates and bisphenol A (BPA), has been linked to reduced testosterone levels in epidemiological studies. Acquired primary hypogonadism is a well-documented consequence of chemotherapy and radiation therapy, particularly when directed at the pelvic region. Chronic health conditions such as type 2 diabetes and liver or kidney disease contribute to testicular dysfunction over time. Obesity, particularly with increased visceral fat, alters hormone metabolism and is associated with lower testosterone levels. Recognizing these influences helps clarify the complex origins of glandular failure.
Biological Drivers of Primary Hypogonadism
Genetic abnormalities play a central role in many cases of primary hypogonadism, with Klinefelter syndrome being the most common, affecting 1 in every 600 male newborns. These individuals typically present with small, firm testes and elevated follicle-stimulating hormone (FSH) levels due to impaired spermatogenesis. Mutations in genes such as *NR5A1* and *INSL3* have also been tied to disrupted testicular development and function.
Autoimmune orchitis, though rare, directly attacks testicular cells, leading to inflammation and progressive hormone deficiency. Some men develop this condition alongside other autoimmune diseases like Addison’s disease or type 1 diabetes. Elevated luteinizing hormone (LH) and FSH levels in the presence of low testosterone confirm primary gonadal failure.
Infections such as mumps orchitis, occurring in about 20–30% of postpubertal males infected with mumps, can result in permanent testicular atrophy in up to half of the affected testes. Chemotherapy agents like cisplatin and alkylating drugs are known to damage germ cells and Leydig cells, reducing testosterone output. Recognizing these biological triggers enables earlier diagnosis and targeted intervention.
Developmental and Acquired Factors that Causes Hypogonadism Development
Congenital conditions such as anorchia (absence of testes) or cryptorchidism (undescended testes) disrupt normal testicular development and function from birth. Men with untreated cryptorchidism face a markedly elevated risk of infertility and hypogonadism, with research indicating up to a tenfold increase in gonadal dysfunction. Exposure to endocrine-disrupting chemicals during fetal development, such as diethylstilbestrol (DES), used between the 1940s and 1970s, has long-term consequences on reproductive health.
Acquired causes include trauma to the testes, which accounts for up to 15% of cases requiring surgical intervention. Radiation therapy for cancers like Hodgkin’s lymphoma, especially at doses exceeding 4 Gy, can permanently impair spermatogenesis and steroidogenesis. Chronic illnesses, such as hemochromatosis, where iron overload damages the testes, and chronic kidney disease, affecting 25–50% of male patients, further contribute to hormonal decline.
Lifestyle factors such as prolonged opioid use, heavy alcohol consumption, and extreme endurance exercise have been clinically associated with suppressed gonadal function. Environmental exposures, including dioxins and polychlorinated biphenyls (PCBs), disrupt hormone signaling pathways. Recognizing these influences is important for comprehensive patient evaluation.
- Klinefelter syndrome (47,XXY) affects 1 in 600 male births
- Mumps orchitis occurs in 20-30% of post-pubertal males with mumps
- Cryptorchidism increases hypogonadism risk up to 10-fold
- Radiation doses > 4 Gy impair testicular function
- 25-50% of men with chronic kidney disease develop hypogonadism
Recognizing the interplay between developmental anomalies and later-life exposures allows for a more precise understanding of individual risk.
Clinical Presentation and Diagnostic Protocols for Hypogonadism

Identifying Physical and Hormonal Symptoms of Hypogonadism
You may notice fatigue, reduced libido, and difficulty maintaining muscle mass if you’re experiencing symptoms of hypogonadism. Men often report erectile dysfunction, decreased facial or body hair, and even gynecomastia due to hormonal imbalances. In adolescents, delayed puberty—such as lack of testicular enlargement by age 14—can be an early red flag. Women may experience amenorrhea, infertility, or hot flashes, especially if ovarian function is impaired. Mood changes like depression or irritability are common across genders, reflecting testosterone’s role in brain chemistry. These symptoms of hypogonadism vary by age of onset and whether the condition is primary or secondary. Persistent low energy and unexplained weight gain may accompany hormonal deficiencies, making clinical evaluation crucial.
Physical signs such as testicular atrophy or low sperm count support suspicion of a hypogonadism diagnosis. Your doctor will assess body composition, secondary sexual characteristics, and signs of hormone deficiency during a physical exam. Hormonal testing typically reveals low serum testosterone levels—below 300 ng/dL in men—on at least two morning blood draws. In women, low estradiol and elevated gonadotropins may point to ovarian failure. Symptoms of hypogonadism often overlap with other endocrine disorders, so a detailed history is key. You should report any past infections, trauma, or chemotherapy, as these can damage gonadal function.
Accurate identification requires distinguishing between primary (hypergonadotropic) and secondary (hypogonadotropic) hypogonadism. Primary forms show high FSH and LH with low sex hormones, indicating gonadal failure. Secondary types present with low or normal gonadotropins and low testosterone or estradiol, suggesting pituitary or hypothalamic dysfunction. Your symptoms combined with lab results guide this classification. For instance, Kallmann syndrome presents with anosmia and delayed puberty due to GnRH deficiency. Recognizing these patterns ensures timely and correct diagnosis.
Standard Diagnostic Evaluations
Blood tests form the cornerstone of hypogonadism diagnosis, with morning serum testosterone being the initial screening tool. You’ll typically need two measurements, taken between 7 and 10 AM, to confirm consistently low levels. Alongside testosterone, labs assess LH, FSH, prolactin, and thyroid function to rule out secondary causes. If prolactin is elevated—above 20 ng/mL—a pituitary MRI may be ordered to check for tumors. These standard diagnostic evaluations help differentiate between hypothalamic, pituitary, and gonadal origins of hormone deficiency.
Additional tests may include semen analysis for fertility assessment or inhibin B levels to evaluate Sertoli cell function. In cases of suspected genetic causes, karyotyping can identify Klinefelter syndrome (47,XXY), present in 1 in 500-1,000 male births. Your doctor might also order iron studies if hemochromatosis is suspected, as iron overload damages the pituitary. Bone density scans (DEXA) are recommended for long-standing cases, as low testosterone increases osteoporosis risk. These evaluations build a comprehensive picture of your endocrine health.
Imaging plays a supportive role in hypogonadism diagnosis when structural issues are suspected. A testicular ultrasound can detect atrophy or tumors, while brain MRI assesses pituitary anatomy. If you have symptoms like headaches or vision changes, imaging becomes critical to exclude adenomas. Standard diagnostic evaluations are tailored to your history, symptoms, and initial lab findings. This stepwise approach ensures accurate classification and guides appropriate treatment planning.
Further details on standard diagnostic evaluations reveal the importance of dynamic testing in complex cases. For example, a GnRH stimulation test assesses pituitary response, helping distinguish hypothalamic from pituitary dysfunction. In males, hCG stimulation tests can evaluate Leydig cell reserve. These specialized assessments are reserved for ambiguous cases where baseline labs don’t provide clear answers. Your healthcare provider uses these tools selectively to confirm the level of hormonal disruption and personalize your care pathway.
Integrative Treatment Strategies for Hypogonadism
Medical science offers structured pathways for hypogonadism treatment, primarily through hormone replacement therapies tailored to individual deficiencies. If your condition stems from primary or secondary hypogonadism, physicians may prescribe testosterone injections, gels, or patches to restore physiological levels. For men, treatment often begins with intramuscular testosterone cypionate or enanthate, administered weekly or biweekly, while transdermal systems provide steady delivery. In cases tied to pituitary dysfunction, human chorionic gonadotropin (hCG) or recombinant gonadotropins may stimulate natural hormone production. These interventions require ongoing monitoring of hormone panels, hematocrit, and prostate health to balance efficacy with safety.
Conventional Medical Interventions
Standard hypogonadism treatment relies on evidence-based pharmaceutical approaches designed to correct hormonal imbalances. Your doctor may initiate therapy with testosterone replacement, available as injections, buccal tablets, or transdermal applications, depending on your lifestyle and absorption needs. For congenital or acquired pituitary causes, treatment often includes gonadotropin-releasing hormone (GnRH) pumps or injectable fertility agents like follicle-stimulating hormone (FSH). Clinical guidelines from the Endocrine Society recommend a regular assessment of serum testosterone, luteinizing hormone (LH), and follicle-stimulating hormone (FSH) every 3–6 months during therapy. These protocols aim to alleviate symptoms such as low libido, fatigue, and muscle loss while minimizing cardiovascular or hepatic risks.
Foundations of Natural Treatment
Dietary and lifestyle adjustments are the cornerstone of natural treatment for hypogonadism, supporting endocrine function without pharmaceuticals. You can enhance testosterone production by prioritizing zinc-rich foods like oysters and pumpkin seeds, as zinc deficiency is directly linked to low testosterone. Regular resistance training, particularly compound lifts, has been shown to increase LH and free testosterone levels within weeks. Sleep optimization—achieving 7-9 hours nightly—supports circadian hormone rhythms critical for gonadal function. Adaptogenic herbs such as ashwagandha (Withania somnifera) have demonstrated efficacy; a 2015 double-blind study found men supplementing with 300 mg daily experienced significant testosterone increases over 8 weeks.
Building on the foundations of natural treatment, consistent circadian alignment plays a major role in hormonal recovery. Exposure to natural light in the morning and reduced blue light at night helps regulate melatonin and cortisol, indirectly supporting gonadotropin release. Chronic stress management through mindfulness or breathwork can lower cortisol, which, when elevated, suppresses the hypothalamic-pituitary-gonadal axis. When combined with targeted nutrition—such as adequate vitamin D from sunlight or supplementation—these practices create a synergistic environment for hormonal balance, complementing both conventional and natural hypogonadism treatment goals.
Alternative and Complementary Therapies for hypogonadism
Acupuncture as a Supportive Measure
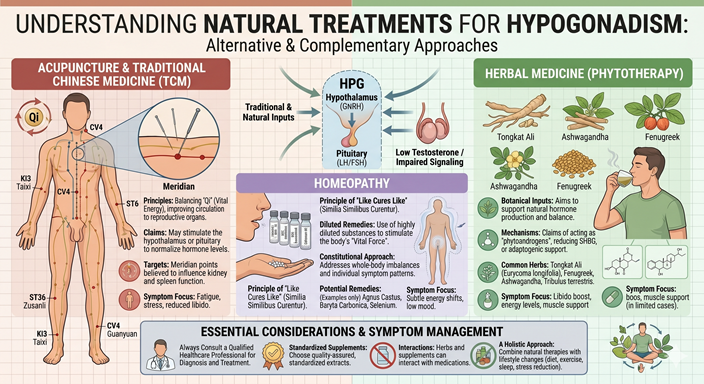
Acupuncture for hypogonadism has been explored in clinical settings as a method to support hormonal balance. Studies suggest that regular sessions may influence the hypothalamic-pituitary-gonadal axis, potentially improving testosterone production in men with idiopathic hypogonadism. You might notice subtle shifts in energy levels and libido after several weeks of treatment, especially when combined with lifestyle adjustments.
Needle placement at specific points like CV4, CV6, and ST36 is believed to stimulate reproductive function. Clinical trials in China from 2018 showed that 60% of participants reported improved symptoms after 12 weeks of twice-weekly acupuncture for hypogonadism. While not a standalone cure, it serves as a complementary strategy alongside conventional care.
Your response to acupuncture for hypogonadism can vary based on underlying causes and overall health. Some patients experience better sleep and reduced fatigue, which indirectly supports endocrine function. Always seek treatment from licensed practitioners with experience in hormonal disorders to ensure safe and targeted care.
Homeopathic Treatment Approaches
Homeopathic treatment for hypogonadism focuses on individualized remedies based on symptom profiles rather than standardized protocols. Practitioners may prescribe remedies like *Agnus castus*, *Selenium*, or *Calcarea carbonica*, depending on your specific presentation, such as low libido, fatigue, or delayed puberty. This system operates on the principle of “like cures like,” using highly diluted substances to trigger the body’s self-regulating mechanisms.
While scientific evidence remains limited, reports and small case studies suggest many patients experience improved vitality and sexual function with consistent use. A 2016 observational study in India noted that 45% of men using homeopathic treatment for hypogonadism reported subjective improvements over six months. These remedies are typically taken in liquid or pellet form, tailored to your constitutional type.
Homeopathy emphasizes holistic assessment, meaning your emotional state, sleep patterns, and digestive health may all influence the remedy selection. This personalized approach differentiates it from many conventional treatments, aiming to restore balance across multiple body systems rather than targeting testosterone alone.
- Agnus Castus 12X: Often used for low libido and premature ejaculation.
- Avena Sativa: Often used for stress-related low testosterone and nervous tension.
- Selenium Metallicum: Used for low sexual desire, weakness, and fatigue.
- Sabal Serrulata & Nuphar Luteum: Used to treat low sexual desire.
- Acidum Phosphoricum & Baryta Carb: It is sometimes used for hair loss associated with hormonal imbalance.
- Damiana & Epimedium: Used for overall male hormonal support.
- Approach: Homeopathy focuses on treating the individual rather than just the symptom, often targeting the “root cause” of reduced hormone production.
- Evidence: These remedies are based on traditional practices and often lack rigorous scientific, FDA-approved studies confirming their efficacy in significantly raising testosterone levels.
- Support: Some proponents suggest that individualized homeopathy might help with subfertility issues
To wrap up
As a reminder, hypogonadism occurs when your testes or ovaries produce little to no sex hormones, affecting fertility, energy, and overall well-being. This condition can stem from problems in the hypothalamus, pituitary gland, or the gonads themselves, with causes ranging from genetic disorders like Klinefelter syndrome to autoimmune diseases, infections, or trauma. Age plays a role too, as testosterone levels naturally decline in men after 30, but clinical hypogonadism involves more pronounced deficiencies requiring attention.
You may notice symptoms such as reduced libido, fatigue, muscle loss, mood changes, or irregular menstrual cycles, depending on your sex and age at onset. While conventional treatments often involve hormone replacement therapy, you have natural options that support hormonal balance. These include maintaining a healthy weight, strength training, ensuring adequate sleep, and managing stress through mindfulness or yoga. Nutrients like vitamin D, zinc, and omega-3 fatty acids also contribute to hormone production.
Your body responds best to consistent, lifestyle-based changes rather than quick fixes. Simple shifts like reducing alcohol intake, avoiding endocrine-disrupting chemicals in plastics, and eating whole, unprocessed foods can make a measurable difference. Always consult your healthcare provider before starting any new regimen, especially if you have underlying conditions. Hypogonadism is manageable, and with informed choices, you can improve your hormonal health naturally.
FAQ

Q: What is hypogonadism?
A: Hypogonadism is a medical condition where the body produces little or no sex hormones due to improper function of the testes in men or ovaries in women. These glands normally make testosterone in males and estrogen in females, which are important for sexual development, fertility, and overall health. The condition can occur at any age and may lead to delayed puberty, infertility, low libido, fatigue, and changes in muscle mass or bone density. It affects both men and women and can stem from issues in the testes or ovaries themselves or from problems in the brain regions that regulate them.
Q: What are the types of hypogonadism?
A: There are two main types: primary and secondary hypogonadism. Primary hypogonadism, also known as hypergonadotropic hypogonadism, occurs when the problem lies in the gonads (testes or ovaries). The glands fail to respond to signals from the brain, even though hormone-stimulating signals (FSH and LH) are high. Secondary hypogonadism, or hypogonadotropic hypogonadism, stems from issues in the hypothalamus or pituitary gland, which fail to send the proper signals to the gonads. This results in low levels of both gonadal hormones and pituitary hormones like LH and FSH.
Q: What causes primary hypogonadism?
A: Primary hypogonadism can result from genetic disorders such as Klinefelter syndrome in men or Turner syndrome in women. It may also follow injury to the testes or ovaries; infections like mumps or orchitis; chemotherapy or radiation exposure; autoimmune conditions; or aging. In some cases, undescended testicles or surgical removal of the gonads can lead to this form. High levels of FSH and LH in blood tests typically confirm that the issue is in the gonads themselves, not in the brain’s signaling system.
Q: What are common symptoms of hypogonadism?
A: Symptoms vary by age and sex. In men, low testosterone can cause reduced facial and body hair, low muscle mass, erectile dysfunction, infertility, fatigue, depression, and decreased bone density. Women may experience absent or irregular periods, hot flashes, vaginal dryness, low sex drive, and trouble conceiving. In children, hypogonadism can delay puberty, leading to lack of breast development in girls or no testicular enlargement in boys. Adults might notice changes in mood, energy, and body composition over time.
Q: How is hypogonadism diagnosed?
A: Diagnosis starts with a detailed medical history and physical exam. Blood tests are used to measure hormone levels, including testosterone, estrogen, FSH, LH, and sometimes prolactin. Low sex hormone levels combined with high FSH and LH suggest primary hypogonadism. Low sex hormones with low or normal FSH and LH point to secondary hypogonadism. Imaging tests like MRI of the brain may be done if a pituitary tumor or hypothalamic issue is suspected. In some cases, genetic testing or semen analysis is also performed.
Q: What natural treatment approaches may support hypogonadism?
A: While natural methods cannot replace medical treatment in most cases, certain lifestyle changes may help support hormone balance. Regular strength training and aerobic exercise can boost testosterone in men. Adequate sleep, stress reduction, and maintaining a healthy weight are crucial factors. Nutrients like vitamin D, zinc, and magnesium are linked to healthy hormone production. Some people explore herbal supplements such as ashwagandha, which has shown potential in small studies to increase testosterone. However, these should never replace prescribed therapy without medical guidance.
Q: Can acupuncture or homeopathy help with hypogonadism?
A: Acupuncture may help manage symptoms like fatigue, low mood, or sleep issues in some individuals, though scientific evidence for its direct effect on hormone levels is limited. A few small studies suggest it might influence gonadotropin release in certain cases of secondary hypogonadism. Homeopathic treatments are not supported by strong clinical evidence for restoring hormone function. Some people report feeling better using these methods, but they should not be used as the sole treatment. Always discuss complementary therapies with a healthcare provider to avoid delays in effective care.
Naturopathic Treatment for Hypogonadism in Philadelphia
If you or someone you know is looking for a more natural approach with minimal synthetic drug use to heal your reproductive functions affected by hypogonadism, the holistic approach might just be what you need or require.
If you suffer from any form of hypogonadism and prefer natural treatment approaches, Philadelphi Holistic Clinic is the right place. At the clinic we have all kinds of holistic techniques residing under one roof.
Contact our clinic at (267) 403-3085 to schedule your appointment for evaluation and treatment. Please consult your OBGYN specialist first and ask if holistic gynecology is the right choice.