HPV (Human Papillomavirus)
Many people encounter human papillomavirus (HPV) in their lifetime, so you should understand its epidemiology, causes, symptoms, homeopathic treatment options, and how to protect your health. HPV is common and usually spreads through sexual contact, though non‑sexual transmission is rare; infections are often asymptomatic but can cause genital warts or cellular changes that affect men and women differently. There is no universally accepted cure; some practitioners use homeopathic remedies and getting significant visible improvement, scientifically documented in different journals.
Key Takeaways:
- HPV is a family of common DNA viruses transmitted mainly by skin-to-skin sexual contact; most sexually active people acquire at least one type during their lifetime (CDC: ~79 million current infections in the U.S., ~14 million new/year; high‑risk types 16/18 cause ~70% of cervical cancers; WHO: ~570,000 cervical cancer cases and ~311,000 deaths/year globally).
- Transmission is primarily via vaginal, anal, or oral sexual contact; less commonly via vertical transmission (mother to baby) or rare nonsexual skin contact—HPV is not caused by poor hygiene.
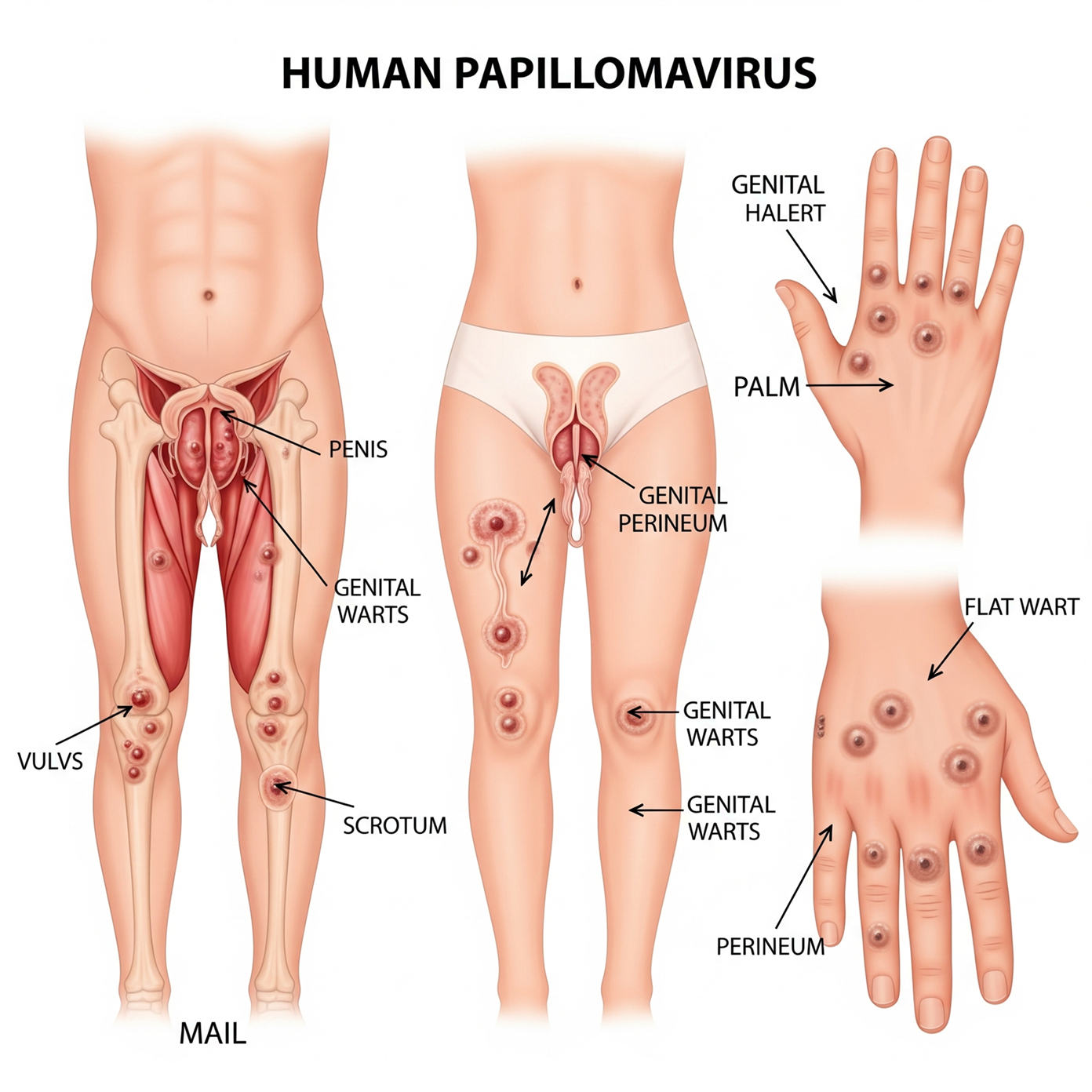
- Most infections are asymptomatic; visible signs include genital warts (soft, raised, or flat bumps on the penis, scrotum, vulva, cervix, or perianal area), while high‑risk types can cause cervical cell changes detected by screening; men may have or subtle flat lesions.
- Screening (Pap smear and HPV DNA testing) is important for women; there is no routine HPV test for men. You can remain sexually active with HPV but use condoms, inform partners, and follow treatment/surveillance guidance to reduce transmission and complications.
- There is no antiviral cure for HPV itself; most infections clear spontaneously within 1–2 years, but persistent high‑risk infection can progress to precancerous lesions and cancer over time.
- Treatment targets lesions and disease: cryotherapy, topical agents, surgical removal for warts, and excisional procedures for cervical dysplasia. Primary prevention is vaccination (nonavalent HPV vaccine), which is highly effective when given before exposure; condoms and regular screening reduce risk.
- Homeopathic remedies (e.g., Thuja and others) and some naturopathic measures are used by practitioners but lack high‑quality evidence to eradicate HPV or prevent progression; they should not replace vaccination, screening, or medical treatments and should be discussed with a licensed clinician.
The Unseen Contagion: Understanding HPV and Its Variants
What Is HPV?
HPV is a family of over 200 related viruses that infect skin and mucous membranes; you will likely encounter at least one type in your lifetime, with studies suggesting most sexually active people acquire HPV at some point. Transmission occurs through skin-to-skin contact, commonly sexual, and many infections are transient and cleared by your immune system within 1–2 years.
The Spectrum of HPV: Types and their Impact
High-risk types like HPV‑16 and HPV‑18 cause about 70% of cervical cancers, while low-risk types such as HPV‑6 and HPV‑11 cause most genital warts; you may be asymptomatic yet still infectious. Persistent infection with oncogenic types raises cancer risk, and vaccination (2-, 4-, and 9-valent formulations) targets the most harmful strains to reduce incidence dramatically.
| Type groups | High-risk (oncogenic) vs low-risk (wart-causing) |
| Common high-risk types | HPV‑16 and HPV‑18—approximately 70% of cervical cancers |
| Common low-risk types | HPV‑6 and HPV‑11—>90% of genital warts |
| Natural history | Most clear in 1–2 years; persistence increases cancer risk |
| Prevention | Vaccination (9-valent covers 6, 11, 16, and 18 + five high-risk types) |
Longer-term data show you can carry a latent human papillomavirus infection for years before lesions or abnormal cytology appear; women screened by cytology and HPV testing have reduced cervical cancer incidence in screened populations. Men often remain undiagnosed because external genital warts or subclinical infection may be subtle; condom use reduces but does not eliminate transmission. Viral load and host immunity affect persistence, and co-factors like smoking or immunosuppression raise progression risk, while vaccines lower both infection and precancer rates substantially.
- You can lower your risk by completing the recommended HPV vaccine series before or during early sexual activity.
- If you develop visible warts, topical or procedural treatments remove lesions but do not eradicate latent virus from tissues.
- Regular cervical screening (Pap/HPV) helps detect high-risk infections early and guides colposcopy when needed.
- Perceiving risk factors like smoking and immunosuppression can help you prioritize prevention and follow-up.
| Symptom variability | Many infections asymptomatic; warts, abnormal bleeding, or lesions in some |
| Testing options | HPV DNA testing, Pap smear, and visual inspection for warts |
| Treatment approaches | Topical agents, cryotherapy, surgical removal for lesions, and monitoring for dysplasia |
| Homeopathic/naturopathic notes | Some use individualized remedies or immune-supportive measures; evidence is limited |
| When to seek care | Persistent lesions, abnormal screening, or concerning symptoms warrant medical evaluation |
The Cold Hard Facts: HPV Prevalence and Transmission
Global and Regional HPV Statistics
About 80% of sexually active people will acquire HPV by age 45; high‑risk HPV prevalence in women with normal cytology is roughly 11–12% worldwide. You should know cervical cancer from HPV causes around 600,000 new cases and ~340,000 deaths annually (2020 estimates), with a disproportionate burden in low‑ and middle‑income countries. Countries with high vaccine uptake (Australia, UK) report up to 90% reductions in vaccine‑type HPV among young cohorts.
Transmission Modes: Beyond the Bedroom
Sexual intercourse is the leading route, but non‑penetrative skin‑to‑skin genital contact, oral sex, and hand‑genital contact can transmit HPV; condoms lower risk but do not eliminate it because infected skin may lie outside the covered area. Vertical transmission at birth can expose newborns, sometimes causing recurrent respiratory papillomatosis, and autoinoculation can move the virus between sites on body.
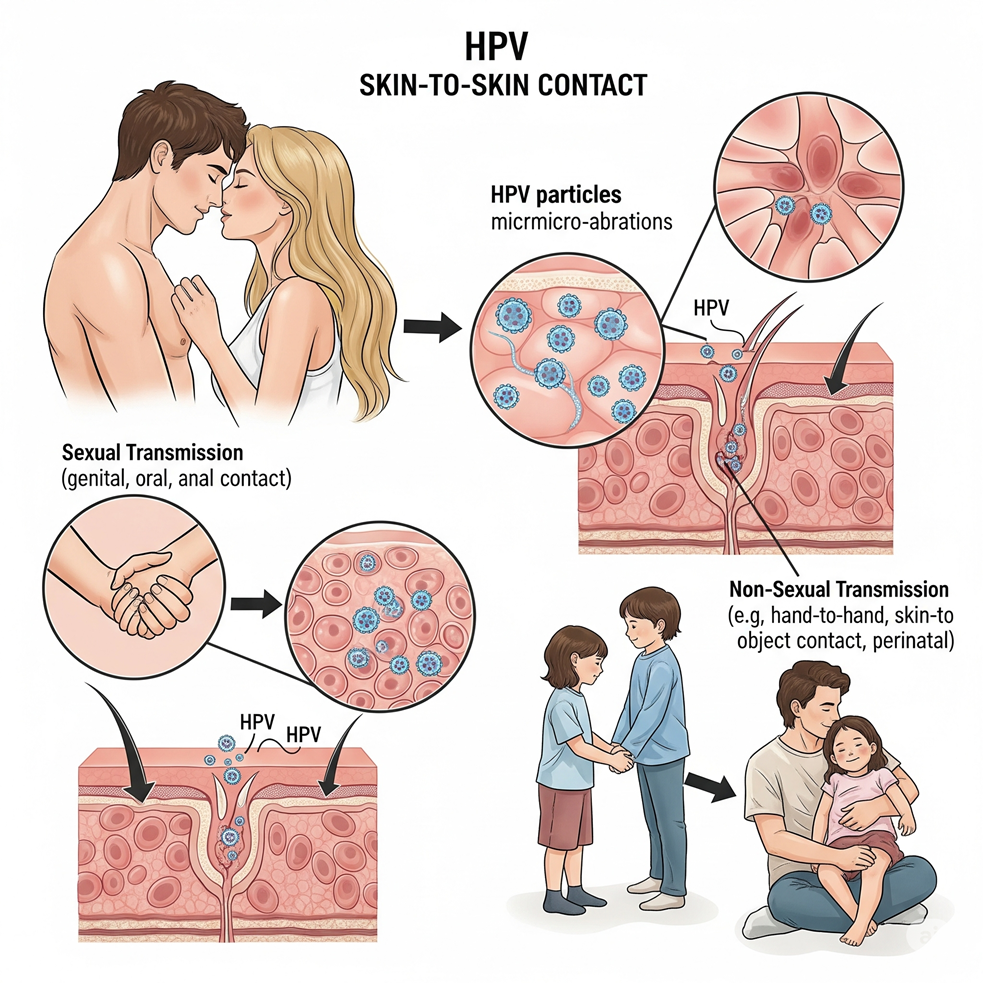
Evidence for fomite transmission is limited: HPV DNA shows up on towels and clinical surfaces, yet detection doesn’t prove infectious virus. If you touch a wart and then another mucosal site, autoinoculation is plausible; postpartum exposure explains several neonatal cases. High vaccination coverage dramatically cuts transmission of vaccine types, producing measurable herd effects in populations where uptake exceeds 70–80%.
The Silent Invader: Causes and Risk Factors of HPV
HPV transmission and persistence depend on a mix of viral characteristics, host immunity, sexual behavior, and environmental exposures; about 79 million Americans are currently infected with human papillomavirus, and roughly 14 million new infections occur each year, concentrated in adolescents and young adults. Major risk contributors include:
- Multiple sexual partners and early sexual debut
- Unprotected skin-to-skin sexual contact (penetrative and non-penetrative)
- High-risk HPV genotypes (notably types 16 and 18)
- Weakened immune system (HIV, immunosuppressive drugs)
- Tobacco smoking and long-term hormonal contraceptive use
- Concurrent sexually transmitted infections that cause local inflammation
This constellation of factors determines your likelihood of acquiring HPV, whether the infection clears, and the risk of progression to precancerous lesions or cancer.
Biological Factors Contributing to HPV
HPV comprises more than 200 genotypes; you face the greatest oncogenic threat from high-risk types 16 and 18, responsible for about 70% of cervical cancers. Viral load and genotype affect transmissibility and persistence, while host immune competence—reduced by HIV or immunosuppressants—raises the chance of chronic infection. Perceiving how viral virulence and your immune status interact helps you understand why some infections clear quickly and others progress.
- Viral genotype (low-risk vs high-risk types)
- Viral load and persistence
- Host immune function (HIV, transplant recipients)
- Age-related cervical epithelial vulnerability (transformation zone in adolescents)
Lifestyle Risks: Habits That Increase Vulnerability
Behaviors that raise exposure or impair local defenses shift odds in favor of persistent HPV: having multiple sexual partners increases exposure exponentially, early sexual activity lengthens cumulative risk, and smoking impairs mucosal immunity and is associated with higher rates of persistence and progression. Perceiving these modifiable habits lets you target prevention and risk reduction.
- Number of sexual partners and partner concurrency
- Inconsistent condom use (reduces but does not eliminate risk)
- Tobacco use (linked to higher persistence and progression)
- Long-term use of hormonal contraceptives (associated with increased risk in some studies)
Population data show HPV is most prevalent among sexually active young adults; vaccination before first sexual contact cuts infection with vaccine-covered high-risk types by roughly 90% in clinical studies. If you smoke, studies indicate roughly a twofold increase in risk for progression to high-grade cervical lesions compared with non-smokers. Oral HPV also stems from sexual practices—oral sex and multiple partners raise oral HPV prevalence, which tends to be higher in men—so combining vaccination, smoking cessation, consistent condom or barrier use, and limiting partners markedly lowers your long-term risk.
The Mask of Normalcy: Symptoms and Identifying HPV
HPV Symptoms in Women: What to Watch For
Most women with HPV have no symptoms, yet you can get genital warts (often from types 6 and 11) or receive an abnormal Pap/HPV test indicating cervical cell changes; types 16 and 18 cause roughly 70% of cervical cancers. Expect cervical abnormalities to develop slowly—months to years—so regular Pap/HPV screening and follow-up colposcopy/biopsy after abnormal results are how early disease is caught and managed.
HPV Symptoms in Men: Signs and Warnings
You will often be asymptomatic, but visible signs include small, flesh‑colored or cauliflower‑like bumps on the penis, scrotum, groin, or perianal area; about 90% of genital warts are linked to HPV 6 and 11. Warts can appear months to years after exposure, and routine urine or penile HPV screening isn’t standard, so partner screening history matters.
Persistent or unusual symptoms should prompt assessment: a non‑healing sore, a lump in the groin or neck, or persistent throat soreness can signal HPV‑related cancers (HPV16 is commonly implicated in oropharyngeal disease). High‑risk groups—men who have sex with men and people living with HIV—may benefit from anal screening and anoscopy; diagnosis relies on visual exam, biopsy, and targeted HPV DNA testing, while vaccination markedly lowers your future risk.
The Warts and the Warring: HPV Warts and Their Management
Understanding Genital Warts: Causes and Characteristics
Genital warts are caused primarily by low‑risk HPV types 6 and 11, which account for roughly 90% of cases; they present as flesh‑colored papules or cauliflower‑like plaques that may be single or clustered on the penis, vulva, perianal area, or cervix. You can experience itching, bleeding, or discharge, yet many lesions are asymptomatic and appear weeks to months after exposure, making the timing of infection often unclear.
Treatment Options for HPV-Related Warts
You can choose patient‑applied options like imiquimod 5% (up to 16 weeks), podofilox 0.5% (twice daily, 3 days on/4 off), or sinecatechins 15% ointment, or provider‑applied methods such as cryotherapy with liquid nitrogen, trichloroacetic acid (TCA), surgical excision, electrosurgery, or CO₂ laser. Vaccination against HPV types 6/11 cuts vaccine‑type warts by about 90% in vaccinated cohorts, while roughly 60% of warts may regress spontaneously within two years.
Imiquimod yields approximately 40–50% complete clearance at 12–16 weeks in trials, podofilox shows 45–60% clearance, sinecatechins about 50–60%, and cryotherapy achieves 50–70% clearance after multiple sessions; recurrence rates vary widely, commonly 20–30% or higher depending on immune status. You should avoid podofilox and use cryotherapy/TCA or surgical options during pregnancy; immunosuppressed people, especially with HIV, often need repeated or combined therapies and specialist referral. Homeopathic remedies like Thuja are used by some patients but lack high‑quality evidence, so integrate them only with close clinical follow‑up and conventional options when lesions persist or complications arise.
The Reality Check: Living with HPV
You can remain sexually active after an HPV diagnosis, but you should use barrier protection and open communication; consistent condom use lowers transmission risk (though not completely), and HPV testing plus Pap smears guide management. Vaccination of partners and eligible people can prevent infection from high-risk strains—Gardasil 9 covers types that cause roughly 90% of HPV-related cancers—while most infections (about 90%) clear spontaneously within two years, shaping decisions on timing and disclosure.
Psychological and Societal Impacts on HPV Carriers
Facing HPV often brings anxiety, shame, or relationship strain because of misconceptions; knowing that 79 million Americans are currently infected and 14 million new infections occur annually can normalize your experience and reduce isolation. Recognize that low-risk types (6 and 11) cause visible warts, while high-risk types 16 and 18 account for about 70% of cervical cancers—facts that help frame risk without stigmatizing you as dangerous or morally judged.
Emotional fallout commonly centers on disclosure and future intimacy: many people delay telling partners or fear rejection, which can increase stress and sexual avoidance. Practical steps reduce harm—seek accurate counseling, use scripted disclosures such as “I tested positive for HPV; most infections clear, and screening keeps us safe,” and consider partner vaccination when eligible. Clinical interventions (Pap/HPV co-testing, colposcopy when indicated) and psychological support like brief CBT or peer support groups measurably lower anxiety; combining medical facts (clearance rates, vaccine efficacy) with communication strategies improves relationships and decision-making.
The Quest for a Cure: Can HPV be Eliminated?
Current Medical Treatments and Their Efficacy
About 70–90% of HPV infections clear spontaneously within 1–2 years, but for persistent or symptomatic disease you can access effective interventions: cryotherapy, salicylic acid, podofilox, or imiquimod for external warts, and LEEP or cone biopsy for high‑grade cervical lesions. HPV vaccines (Gardasil 9) prevent the HPV types responsible for roughly 70–90% of cervical cancers when given before exposure, and screening plus treatment of precancerous lesions has driven major declines in cervical cancer incidence.
Naturopathic and Homeopathic Approaches: Do They Work?
Conventional medicine regards warts resulting from HPV infection as a surgical matter. Cauterization or surgical excision of warts is primarily advised by them. The outcomes of these treatments are transient and pose a danger of scarring. Homeopathy adopts a delicate and moderate methodology in addressing HPV infections that result in warts. In scientific studies, homeopathy effectively and naturally addresses warts caused by HPV. Homeopathic remedies enhance the body’s intrinsic immune response to eliminate warts at their source. The homeopathic therapy modality provides an efficacious remedy for HPV-induced warts, devoid of adverse side effects. In contrast to traditional medicine, homeopathy does not suppress symptoms, rendering it an optimal therapy choice for human papillomavirus infection. Scientific research proves the effectiveness of this method. Case reports published in scientific journals show an effectiveness and absence of adverse effects.
Human Papillomavirus Treatment with Homeopathy
One of the most widely used holistic medical approaches is homeopathy. Using a holistic approach, the solution is chosen based on the individualization hypothesis and the similarity of symptoms. Eliminating all of the signs and symptoms that the patient is experiencing is the only method to restore them to a state of full health. Treatment options for human papillomavirus (HPV) symptoms can be chosen based on the complaints’ origin, location, sensation, modalities, and severity. The following list of crucial treatments for human papillomavirus (HPV) symptoms includes:
Thuja, Dulcamara, and Causticum
Homeopathic remedies for HPV-induced skin warts include Thuja, Causticum, and Dulcamara. Thuja and Causticum are effective for substantial, irregular warts. These warts may exhibit tenderness upon contact and may occasionally hemorrhage. Thuja and Causticum are beneficial for pedunculated warts. Dulcamara is regarded as the most effective treatment for HPV-associated flat and smooth warts. Dulcamara is quite effective for warts manifesting in crops.
Thuja.
Arousal level high. The vulva and perineum may develop warty growths. A thick, greenish leucorrhea that is profuse. Extreme discomfort in the left inguinal and ovarian regions, as well as gonorrhea. The testicles constantly indurate. I have a strong need to urinate often and intense pain when I am approaching the neck of my bladder. Crucial symptoms include spongy tumors, warty excrescences, enlarged prostate, and condylomata. Mucous tubercles that are moist.
Causticum.
Pain, redness, and inflammation are common symptoms. Large, sharp, easily-bleeding warts
Dulcamara
Flat, big warts and sharp discomfort around the navel. Swelling and enlargement of inguinal gland.
Natrum Sulphuricum and Nitric Acid
Effective treatments for HPV infection resulting in genital warts in men include Natrum Sulph and Nitric Acid. Natrum Sulph is most effective for warts located on the penis and scrotum. Pruritus and unease are frequently evident. Nitric Acid is one of the most commonly prescribed treatments for HPV in males with highly sensitive genital warts. This illness is predominantly characterized by burning and pain. The individual reports experiencing splinter-like agony. Genital warts that exhibit bleeding upon contact indicate the necessity for a prescription of Nitric Acid.
Natrum Sulphuricum.
Experiences changes in moisture levels; prone to warts. After a woman has gonorrhea, her leucorrhea turns yellowish-green. The patient is experiencing leucorrhea along with hoarseness. Infestations of yeasts; red bumps all over the body resembling warts.
Nitric Acid.
Hydrogenoid constitution. Sycotic remedy. Discomfort and redness in the glans and under the prepuce. Wounds that ooze, hurt, sting, and produce an unpleasant odor. Hair on the vaginal area thinning
Mercurius Solubilis.
Feeling of rawness in certain areas. Ovaries discomfort (Apis). Itching and burning; increases after going to the bathroom; alleviates after a cold shower.
Empowering Prevention: Strategies to Avoid HPV Infection
Vaccination: The Key to Prevention
Gardasil 9 protects against nine HPV types, including HPV‑16/18, which cause about 70% of cervical cancers, and additional types that together account for roughly 90% of vaccine-preventable cervical disease. You should vaccinate at 11–12 years (two doses) and complete the series before sexual debut; routine catch-up is recommended to age 26 and individual assessment up to 45. High-coverage programs have reduced cervical pre-cancers by nearly 90% in vaccinated cohorts.
Safe Practices: Sexual Health Tips
Use condoms consistently to lower transmission risk, while recognizing HPV spreads via skin-to-skin contact, so condoms are not fully protective; limiting sexual partners and choosing long-term monogamy reduces cumulative exposure. You can ask partners about vaccination and get regular cervical screening—Pap every 3 years (21–29) or co-testing every 5 years (30–65)—since over 80% of sexually active people acquire HPV during their lifetime.
- Use condoms and dental dams correctly for vaginal, anal, and oral sex.
- Encourage partner vaccination before sexual activity to reduce mutual risk.
- Share sexual history and consider staggered testing before becoming sexually active together.
- You should attend routine screenings and follow your clinician’s testing schedule.
HPV is often transmitted from asymptomatic partners; many infections clear within 1–2 years, but persistent high‑risk types can cause CIN and cancer if undetected. You should avoid tobacco—smoking increases viral persistence and progression—and disinfect or avoid sharing sex toys, use barrier protection for oral sex, and keep immunizations and screenings up to date to catch precancerous changes early.
- Limit new or concurrent partners to lower exposure probability.
- Get vaccinated and confirm partner vaccination status before sex.
- Maintain on-schedule Pap/HPV screening and follow-up for abnormal results.
- You should quit smoking to reduce the chance of persistent infection and progression.
Summing up
So HPV is a very common sexually transmitted virus that often causes no symptoms but can produce warts or, in persistent high-risk types, precancerous lesions; you can acquire it through skin-to-skin sexual contact and rarely nonsexual means. If you notice symptoms, seek medical evaluation; conventional prevention (vaccination, condoms, screening) reduces risk. Homeopathic remedies are used by some professionals as supportive care; consult qualified clinicians to combine approaches safely.
FAQ
Q: What is human papillomavirus (HPV), and how common is it?
A: HPV is a group of more than 200 related DNA viruses that infect skin and mucous membranes. Types are classed as low‑risk (cause warts) or high‑risk (can cause cancers). HPV is extremely common: most sexually active people acquire at least one HPV type in their lifetime. High‑risk types 16 and 18 are responsible for about 70% of cervical cancers worldwide; overall lifetime exposure estimates often exceed 70–80% in sexually active populations.
Q: How is HPV transmitted, and can it be transmitted non‑sexually?
A: HPV is primarily transmitted by direct skin‑to‑skin contact, most often during vaginal, anal, or oral sex. Genital area contact without intercourse can transmit HPV. Non‑sexual transmission is uncommon but possible: perinatal transmission from mother to baby during delivery can cause respiratory papillomatosis; fomite (via objects) is considered rare. Asymptomatic people can still transmit the virus.
Q: What causes HPV infection, and what are the main risk factors?
A: Infection is caused by exposure to infectious HPV particles. Risk factors increasing acquisition or persistence include having multiple sexual partners, early onset of sexual activity, unprotected sex, compromised immune function (HIV, immunosuppressants), smoking, and long‑term use of oral contraceptives (associations exist). Persistent infection with high‑risk types can lead to precancerous changes and cancer over years to decades.
Q: What are the symptoms of HPV in women and men, and what do warts look like?
A: Most HPV infections are asymptomatic. Low‑risk HPV can cause visible warts: genital warts (condylomata acuminata) are flesh‑colored or whitish, raised or flat, and sometimes clustered with a cauliflower appearance; they can appear on the vulva, vagina, cervix, penis, scrotum, groin, or perianal area. High‑risk HPV infections usually cause no early symptoms but can produce abnormal cervical cytology, and over time may lead to precancerous lesions or cancers (cervical, anal, oropharyngeal, penile, vulvar, or vaginal). In men, warts or small bumps on the penis, scrotum, or perianal area are common visible signs; many infections remain invisible.
Q: Is Human Papillomavirus curable? Can you get rid of it once you have it?
A: There is no antiviral that reliably eradicates HPV from the body. Most HPV infections clear spontaneously within 1–2 years due to the immune response. Treatment targets visible lesions (warts, precancerous cells) rather than the virus itself. Persistent infection with high‑risk types requires monitoring and treatment of precancerous lesions to prevent progression to cancer.
Q: What evidence‑based medical treatments exist, and what about homeopathic or naturopathic options?
A: Evidence‑based treatments for visible warts and precancerous lesions include cryotherapy, topical agents (imiquimod, podofilox, podophyllin, and trichloroacetic acid), surgical removal, and, for high‑grade cervical lesions, excisional procedures (LEEP and cone biopsy). Prophylactic HPV vaccines (bivalent, quadrivalent, and nonavalent) prevent infection with common high‑risk and wart‑causing types and are highly effective when given before exposure. There is no high‑quality evidence that homeopathic remedies clear HPV or prevent progression to precancer; commonly cited remedies in homeopathic practice (e.g., Thuja) lack reliable clinical proof. Some people use naturopathic measures (immune‑supportive lifestyle, micronutrients) as adjuncts, but these should not replace vaccination, screening, or medical treatment for lesions.
Q: How can HPV be prevented, and what screening is recommended?
A: Primary prevention: HPV vaccination according to national guidelines (recommended before sexual debut, and in many programs up to mid‑20s or older in specified groups) is the most effective prevention. Safer sex practices (condom use) reduce but do not eliminate risk. Limiting the number of sexual partners and smoking cessation lower the risk of persistent infection. Secondary prevention: regular cervical screening (Pap smear and HPV testing) as recommended for age groups and follow‑up of abnormal results. Pregnant women with HPV should discuss management with their provider; delivery decisions are guided by obstetric indications rather than HPV alone.
Homeopathic Treatment for HPV
It is advisable to seek professional medical assistance if you are diagnosed with HPV.
At Philadelphia Homeopathic Clinic, internationally recognized homeopaths, Dr. Tsan and associates, deliver natural treatment for the main cause of human papillomavirus.
Contact our clinic at (267) 403-3085 to schedule the initial homeopathic evaluation.